clinical case: Young Lady, breaking the scapholunate ligament right wrist.
[clinical case 2 - Christophe Mathoulin - EWAS 2015]
Born 21-02-1982 she received emergency at 3 months with direct surgical repair (Anchor into lunate, with pinning).
2004, falling down stairs, breaking the scapholunate ligament Right wrist.
She received emergency at 3 months with direct surgical repair (Anchor into lunate, with pinning)
Failure of direct open suture!
After the non-improvement in April 2004, the second intervention took place in December 2004 to modified Brunelli ligamentoplasty
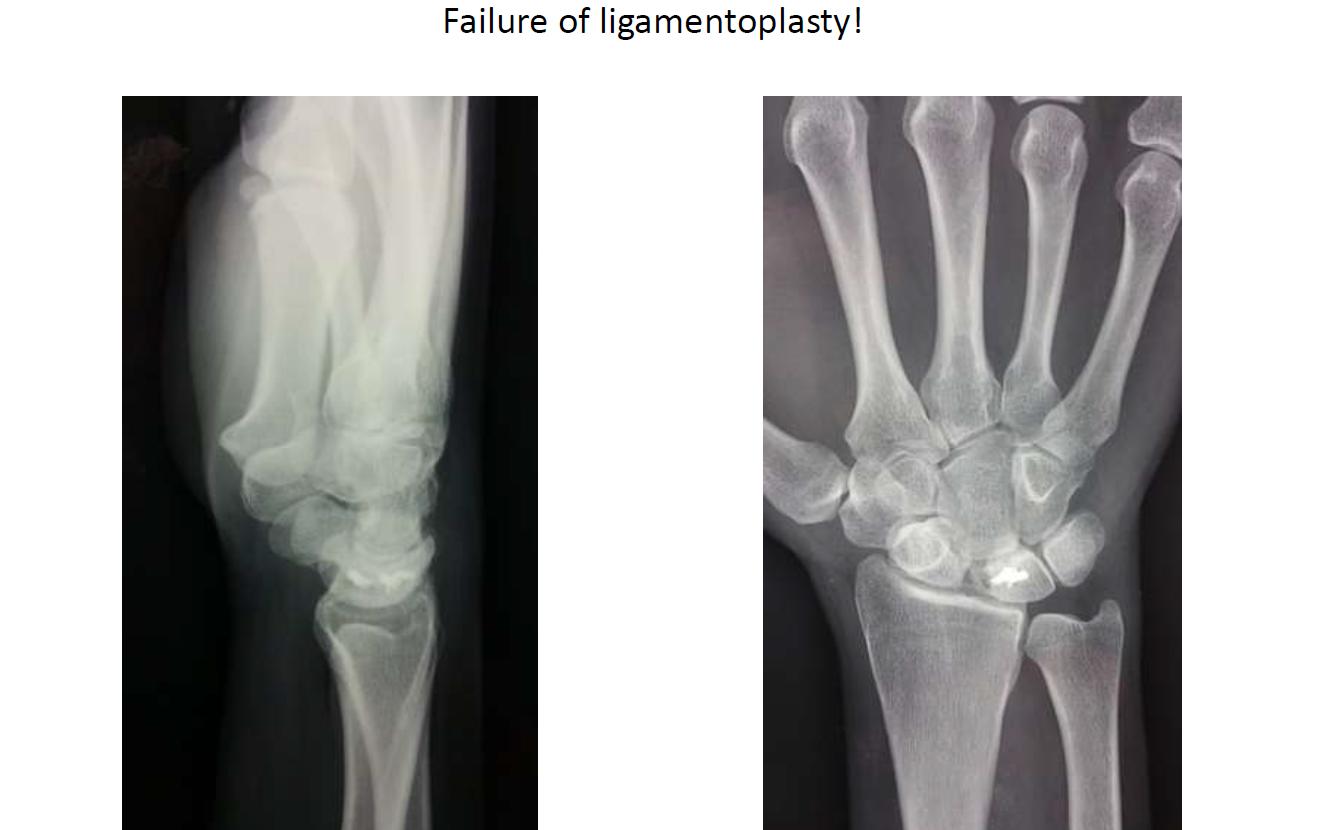
Failure of ligamentoplasty!
In 2006, Four bone fusion, Progressive Radio-carpal osteoarthritis
Currently it has relatively well preserved mobility
- Extension 60 against 85
- Flexion 55 against 85
- IC 30 against 40, IR 20 against 30
- Full pronation-supination
- FM 10 kgf against 30
- Pain VAS 9 to 10
- Dash 68.18
Dear friends
Please let me know what will be your proposal regarding on this case !!
Prof. Christophe MATHOULIN
France
PDF files
contactez nous
2016 medical discussion
Dear Christophe
My proposal in such cases is a capitate resurfacing procedure with the CMI pyrocarbon implant
Because she is very painfull and still has a good wrist range of motion
Nicolas Dreant Nice France
Wow, what a challenge at that young age with that amount of pain, Christophe 
How about denervation?
Ilse Degreef Belgium
If the patient has pain would perform a wrist arthroscopy to classify the lesion.
The treatment options could be :
1)Arthroscopic debridement and ligament suture of dorsal remanent and cast 6-8 weeks
2)Arthroscopic debridement and inmovilization with cast 6.8 weeks
3)Arthroscopic debridement and E-L pinning for 6 to 8 weeks
Greetings from Buenos Aires
Alvaro Muratore
Buenos Aires
For me Total wrist denervation. To young for a prostheses or Total wrist arthrodesis.
Pr M. LEVADOUX - France
soft tissue procedures have already failed, better if plan B is not the same as plan A, 10yrs after there is not going to be much remnant of anything; the case has reached the stage of skeletal reconstruction, but not quite clear from the outline what "indication" is asked for ?!;
if it is intractable pain (dorsal ? ulnar ? radial ?) it will likely boil down to the usual pain vs. motion decision (after poss. playing around a while with denervations, arthroscopic debridements and the like) ...
Arno R. Schleich MD
Plastic Surgery, USA
I think that is possible to try wrist denervation, because the patient is too young and she has a very good ROM. Best regards
Carlos Morales Sanchez-Migallon
Apologies for the previous answer, i had not seen the whole case.
In Argentina is very difficult get prostheses therefore the only options that could provide for a patient with a lot of pain are:
1) Interposition with dorsal capsule
2) Total wrist arthrodesis
As the patient has good mobility it could try a wrist denervation but personally I have not had good results with wrist denervations.
Alvaro Muratore
southern france's school, as M Levadoux, I'd try to gain a few years with a total denervation. Eventually in addition with hyaluronic injection
Andre Gay France
What a case.
Christophe, I bet you would love to have a time machine and perform your arthroscopic DCSS repair at the first moment, don't you?
Well, back to reality... I also bet the denervation was already done on the second or third surgery... most surgeons do it, no?
I had recently a case very similar. Same evolution, 2 prior surgeries elsewhere, then I did a 4 courner, and then I had a nonunion and then I revised the 4 courner... And 3 years after, she started with pain and radio-lunate arthritis...
In my case, as in this one, I notice arthritis is more on dorsal part with dorsal osteophite on radius, typical of dorsal impingement after the 4 corner. Probably is more painfull during wrist extension on dorsal aspect, is it?
I performed in such case an arthroscopic ressection of dorsal margin of radius, including osteophite. The patient improved the pain, specially on weight bearing during wrist extension (1 year ago, so far so good). It may be paliative but for such young patient may be a choice for now... Dr. Gustavo Mantovani Ruggiero
Cirurgia da Mão e Microcirurgia Robotica
At the risk of sounding out of sorts after there have been so many treatment suggestions, I think it is essential to provide the forum members with the clinical symptoms and signs in order for them to make sensible decisions. After all we treat patients and not x-rays/scan and it is not possible to advise treatment based on the imaging alone. I presume she has pain arising from the radiocarpal joint, but if so, this should be made clear.
To highlight this, what if the patient had intersection syndrome or another condition and the advice is to perform a wrist replacement!
Best wishes
Robert Farnell
Well...vas and dash do tell a lot here on the clinical impact of the radiological findings, no? ?
Ilse Degreef
I agree with Michel Levadoux. Denervation to safe time. Too young for prosthesis and too good motion for arthrodesis
Alvaro: wrist Prosthesis are available in Argentina. Re Motion is in the local market, though expensive for us.
Pablo De Carli
download all discussion on the PDF file discussion clinical case, and improove yourself.
| 

 basculer vers :
basculer vers :

















 discussion clinical case.pdf
discussion clinical case.pdf
 MedTools support :
MedTools support :