One of us young colleague presented a foveal detachment of the TFCC
[clinical case 3 - Christophe Mathoulin 2016]
Case:
difficult case. One of us young colleagues (23 yo) presented a foveal detachment of the TFCC. He was operated a few months ago by open procedure with a somewhat curious technique.
The surgeon used a hemi-band of the ECU, left attached to its distal insertion, passing through the TFCC and then into a tunnel in the head of the ulna (but it is not the technique described by Toshi with a tunnel from fovea to ulnar side of ulna and fixed proximally.
In this case it was a tunnel from fovea to radial side of ulna and fixed to itself dorsally ?!)
This results in the maintenance of a dorsal dislocation of the ulnar head with limitation of supination very troublesome in this young orthopedic surgeon.
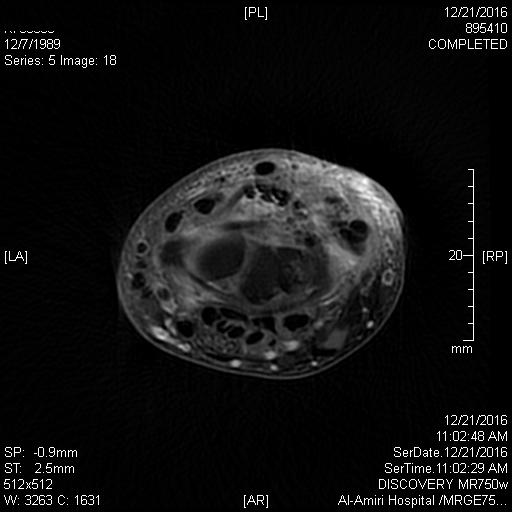
You will see on the axial MRI images starting from image 1 the most distal to image 3 at the ulnar head, the separation into two strips of the ECU. On the saggital images we see the dorsal dislocation of the ulnar head.
In summary:
Ulnar head dorsally subluxed (the palmar portion of DRUJ is filled with fibrosis)
The principle of the ECU plasty always attached in its distal part to its dorsal insertion on the basis of the 5th metacarpal stabilizes the dorsal luxation
The dorsal capsule appears fragile and weak
What do you think? What therapeutic proposal?
Christophe MATHOULIN
reference publication
Anatomic Foveal Reconstruction of the TriangularFibrocartilage Complex With a Tendon GraftGregory I. Bain, MBBS, FRACS, FA (Orth) A, PhD,*wzDuncan McGuire, MBBCH, FCS (Orth), MMed,*wYu Chao Lee, MBBS,*wKevin Eng, MBBS, FRACS,*wand Matthias Zumstein, MDy
contactez nous
Hi Christophe,
Im not totally sure, but it is a hybrid of Toshi’s technique and the one described by Hayes and Goldner in about 1988 (ECU through the ulnar head and back onto itself).
The technique that we have used is to put a mattress suture of palmaris (or could be free graft of ECU) through the ulnar TFC to the fovea.
I have included a paper on a technique we published in 2014 [Here]
I have changed the way I do it now, I now deliberately excise the ulnar styloid, which is easier, safer and provides the best fixation with a screw in anchor I have seen
Greg Bain, South Australia
When the bone tunnel was made from fovea to the radial ulnar neck, it is a little bit difficult to tighten the TFCC when the ECU half-slip was pulled. So, I think in this case, the TFCC was not enough reattached to have enough reduction of the DRUJ.
When the ECU-half-slip was sutured back to itself, the next issue is expansion of the bone tunnel.
At this moment, the patient should be carefully done by prono-supination exercise with bandage wrapping around the DRUJ.
If your colleague will have dorsal subluxation or DRUJ instability after the therapy, and If his ulna shows positive ulnar variance, you can shorten the ulna to tighten the TFCC.
Regards
Toshiyasu Nakamura, Japan
Interesting case. I may be misunderstanding the technique but I'm not convinced that it restores the TFCC insertion to the ulna.
Is it possible that the ECU graft itself may be maintaining the dorsal subluxation.
I'd be interested in knowing what happens in supination- if he can supinate. Would it be worth getting another MRI with the wrist in supination?
I see no harm in hand therapy to work on strengthening secondary stabilisers. It worked very well with my TFCC detachment!
Andrew mahon
Interesting case Mathu. I had a similar case a lot of years ago with the same problem. I did a new open surgery removing the part of the ECU tendon used to fix the TFCC to the ulna and I fixed the ulnar part of the TFCC to the fovea. In this case the TFCC was good in quality and patient healed even with some discomfort in the ulnar side of the wrist. Actually I suggest to verify the quality of the TFCC ligament before to decide which tipe of surgery use and the Adams technique is a choice when the the ligament is degenerated. The Bain technique is a good alternative but I think that a sufficient good quality of remanent TFCC ligament is needed.
good luck.
Riccardo Luchetti
It seems a nice indication for the DIOM reconstruction technique we've been performing here at Sao paulo on the last 3-4 years with nice results.
The final manuscript is about to be sent for publication. We use a variation of a technique published on JWS that used the PL, but in our case we use the BR. This technique do not depend on good TFC tissue and dorsal capsule. We keep the distal insertion of the BR attached to radius styloid, harvest the tendon till its transition to muscle, and drill a 3.5mm tunnel obliquely from 3 cm proximal to BR attachment aiming the ulna head, crossing the interosseus membrane in the middle just proximally to the DRUJ, obliquely (more proximal on radius and more distal on ulna), and fixing the tendon on the ulna head with a Arthrex 3.0 screw of biotenodesis. i sent some pictures of this technique in this forum before.
Gustavo MantoVani
Brazil
may I suggest to put something on the dorsal part of the bald head of the ulna. The ECU in continuity can be deviated on the head of the ulna and kept in this place by a slip of half of the retinaculum like we do in rhumatoid arthritis. I would remove the part of ecu in the joint if it limits supination and put it back to original tendon deviated.
best regards
Bernard Cadot, Antony, France
| 

 basculer vers :
basculer vers :


















 MedTools support :
MedTools support :